It was in early July 1964 when I had just begun a three-year psychiatry residency at Oregon Health and Science University (OHSU), previously the University of Oregon Medical School in Portland, Oregon. It was the first time I was assigned to a hospital ward designated solely for psychiatric patients and within the first week of the residency I became painfully aware that I did not know what I was doing. During the second week of the residency the chief of psychiatry became professionally aware that I did not know what I was doing. In the presence of the three other first year residents and the third-year resident, during my description of my patients, he said, “Ken, you do not know what you are doing!” I replied, “I know that. I have no idea what I am doing. I was hoping I would learn my way as to how to be a psychiatrist.” He turned to the third-year psychiatrist and said, “Take Ken under your wing until he knows what to do.”
I continued following the outline for psychiatric evaluations. The myriad information we were to acquire from patients did not seem to funnel into any formula or template. Further, it seemed that the psychiatric evaluation gave the patient’s medical and surgical history less than equal attention. I hoped I was wrong in that perception. I became apprehensive I might have to forfeit my accumulated medical knowledge and experiences in order to become a psychiatrist. I had four years of medical school, one year of rotating internship, one year of surgical residency, one year of neurology residency, and three years stationed in France carrying out general medicine and neurology for the Medical Corps of the United States Army. I began feeling anxious, depressed, and sometimes I did not sleep well. I felt chagrined about not completing the two former residencies and now I was feeling uneasy with this residency in psychiatry. I decided to stick it out, however, hoping for a solution. The third-year resident did review each one of my psychiatric evaluations and made some suggestions, but I did not mention my thoughts and fears to him.
One of my patients was a child who was blind, whose residence for each grade school year was the Oregon School for the Blind in Salem, Oregon. As a result of this connection I was invited to join the faculty at one of their conferences being held in Lincoln City at the Pacific coast. The faculty felt challenged to get a handle on all the different activities their students did on and off campus. It seemed similar to my attempt to get a handle on the myriad information per psychiatric patient.
When I wrote up the medical and surgical history for each patient I used the formula familiar to all physicians, the Review of Systems, created by a German physician, Rudolph Virchow. Here are a few of these familiar systems in our body: cardiovascular (heart and blood vessels), gastrointestinal (digestive), musculoskeletal (muscles and skeleton) , skin, and neurological (brain and nerves). Each system is examined as to: normal, deficient, excessive, maladaptive, or obsolete behavior. Behavior is what someone or something is doing. Thanks to Virchow two amazing things occurred to me and it was the answer to my prayer. I became very excited. I felt that I finally had a formula for psychiatry that adequately included medical and surgical history. I stopped experiencing anxiety, depression, and insomnia.
If the human body can be divided into systems and examined for behavior why not divide human activity into areas and examine these areas for behavior?
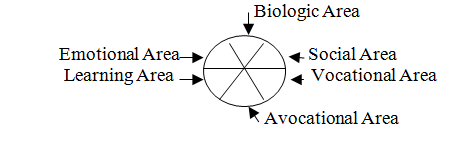
I came up with six areas and called it the Review of Areas© . I drew a circle. Using this Review of Areas© formula or template I could sort the patient’s myriad information into six areas of behavior: biologic, social, vocational, avocational, learning, and emotional. I could give each area the attention it deserved.
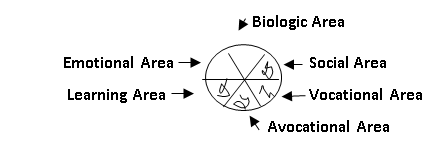
Not long after, I was on a three-month rotation at one of the state hospitals in Oregon. Each one of my 15 or so patients gave me permission to share his or her Review of Areas circle on a 4“x 5” page from a memo pad with the other patients. The nursing staff let me tape their pages on a seldom used window at the nurses’ station. The patients gathered around this window to compare their circles. They were startled that the majority of their pie diagrams were similar: “behavior” in only two of the six areas: biologic and emotional.
Upon returning to the medical school I continued the same bulletin board idea. The nurses began calling the Review of Areas© diagram “Paltrow’s Pie.” And then one of the residents asked me if I planned to get it published. I told him I had not considered it, I had not written any articles for medical journals, and that I did not have the skill for writing. He told me he thought the Review of Areas© was a valuable formula, that he had written articles that had been published, and he would like to assist me in writing this article. I accepted his assistance.
For the subject of the article I chose a patient who, many years before, was injured during a fall into an open manhole. He then underwent a number of operations. For four years he received physiotherapy from an orthopedic surgeon. Then for 2 ½ years he was treated by a psychiatrist for anxiety, depression, delusions, and suicidal thoughts. When he became my patient on the psychiatric ward at the medical school hospital I carried out my Review of Areas© formula for information. After I prescribed psychiatric medication I showed him the diagram. Like the others before, he was “behaving” in just two areas: biologic and emotional. I sought help for his deficient social area: he began taking walks with his wife, met with neighbors, spent more time with his brother, and resumed attendance at union meetings. For his deficient vocational area his union representative placed his name on a job availability list taking into consideration his physical limitations. For his deficient avocational area he resumed his hobby of wood carving. He avoided his deficient learning area choosing not to study or learn any new subjects. The outcome was that he did return to his trade as a machinist. He had ceased being suicidal. He had stopped experiencing delusions. His pain gradually decreased as did his anxiety and depression. His self-esteem increased. Medication was gradually reduced and essentially discontinued.
We submitted the article to a medical journal and it was accepted for publication in 1967. (1) I received many postcard requests for reprints, many from around the world.
Consider the law of conservation of energy. Energy can be converted, transferred, and transformed. I was intrigued that this Review of Areas© formula offered a picture of a person's transference of energy. Deficient use of energy in one or more areas simply transfers or shifts energy to other areas. For example, deficient expenditure of energy in one's social, vocational, recreational, and learning areas results in excess expenditure of energy in one's emotional and biologic areas. Common sense and reason support efforts to revive use of energy in deficient areas. Creating (or re-creating) behavior to be as normal as possible in as many areas as possible could reduce anxiety, depression, delusions, pain, and suicidal ideation, and in return increase one’s self-esteem and productivity.
In 1980 I took advantage of my continuing expertise in the Review of Areas© to update it with two name changes: “biomedical” for biologic and “recreational” for avocational. (2) And again, I received requests for reprints from around the world.
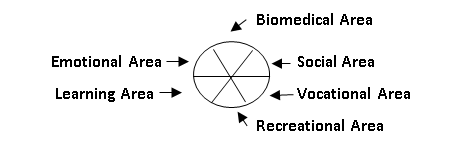
My update included details for each area that could be looked at for normal, deficient, excessive, abnormal, or obsolete behavior including:
- Biomedical area: review of systems, current symptoms to include hallucinations and delusions; history of illnesses, accidents, operations and other treatment, and family medical/surgical history, etc.
- Social area: family, relatives, friends, marriage/divorce, social organizations, anniversaries, economic status, legal history, government, cultural background, geography, pets, and animals, etc.
- Vocational area: current vocation and history of vocation to include military service, and the labor involved carrying out activities of daily living, etc.
- Recreational area: hobbies, interests, pastimes, activities of play, spectator activities; and two new interpretations--to be creative and to re-create.
- Learning area: history of formal education, informal education, and self learning.
- Emotional area: feelings and emotions that pertain to the present, the past, and the future? And how are these feelings handled? An addition for this area could be a description of personality.
Yes, I stayed with this residency. The Review of Areas formula made all the difference and I continue to use it in my practice to this day.
(1) Paltrow KG, Brophy JJ. “Review of areas: A Key to diagnosis.” Postgraduate Medicine 42: A 137-A 141, December 1967© McGraw-Hill, Inc.
(2) Paltrow KG. “Review of areas: Updated method of patient evaluation.” Postgraduate Medicine Vol 67/NO 1/Jan 1980: 211-215 ©McGraw-Hill, Inc.