During my third year of residency in psychiatry I was assigned to the hospital outpatient liaison service. It was my role to respond to requests from the other specialties to carry out timely psychiatric consultation service. One afternoon a resident in obstetrics and gynecology (OB/GYN) contacted me to consult on a crisis.
A forty-year-old female patient had come in two weeks before for more than the usual checkup for breast or cervical cancer. She had pigmentary changes around her nipples, enlargement of her abdomen, cessation of menses, and morning sickness and was absolutely certain she was pregnant.
Even though the physical examination did not support the diagnosis of pregnancy the resident ordered the standard laboratory pregnancy test. During this follow-up visit in the clinic he told her she was not pregnant. This made her angry. She was adamant that she was pregnant. She had never been a mother and this was her one and only opportunity. Then, suddenly her anger turned into despair. If she was not pregnant she no longer wanted to live.
The resident diagnosed her disorder that of pseudocyesis, a false pregnancy, one of the somatoform disorders. She had a delusion about her soma, the organic tissues of her body. Thus, the resident had a psychiatric crisis on his hands. I told this resident I would evaluate his patient in the OB/GYN clinic within the hour.
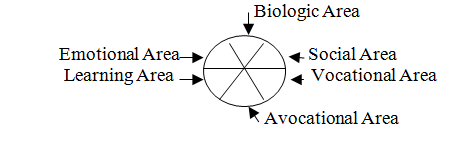
Before meeting her I looked at the Biomedical Area in her chart and found no additional information of merit and I knew her major emotions. So I would gather information as to her behavior, what she had or had not been doing, in her social, vocational, recreational, and learning areas.
I introduced myself. She was courteous, controlled her emotions, and indulged my questions knowing that no matter what I found or diagnosed she would not budge from her belief that she was pregnant.
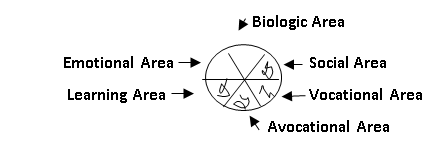
I was not surprised to discover that she had no social life with family or others, was not working, had no meaningful recreation or hobbies, and was not attending school or interested in current affairs. I wrote a brief note in the outpatient chart along with my hand-drawn ROA circle, her behavior x-ray, demonstrating deficiency in four areas. At my request she said she would remain in the OB/GYN clinic while I called the resident.

I told him that the pseudocyesis was being fed by her metabolic energy, as this energy was totally confined to her emotional and biomedical areas. If we rejected her delusion she would probably take her life. Medication was out of the question because she would fear it would harm the fetus. The solution lay in integrating psychiatry and obstetrics.
We needed to stall confronting her with the truth. The resident would tell his patient that he wanted a second pregnancy test to be certain. During the two-week interim for the test results his patient would attend an outpatient psychiatric group therapy that met twice a week. Hopefully, her metabolic energy would be diverted from fueling her delusion to fueling her revived social area.
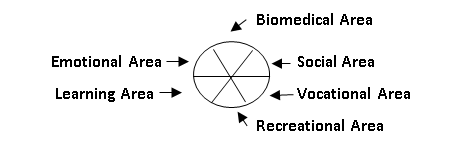
Two weeks later the OB/GYN resident called me. Before he could tell his patient that the lab test was again negative she blurted out that she hoped she was not pregnant. She was making friends in the group. She learned from them that it would be difficult for someone at her age of forty to raise a child on her own. A few lived near her so they were setting up plans to do things together. The group therapy gave her useful social behavior, which would undoubtedly expand to include recreational and possibly voluntary vocational behavior.
Here is the final behavior x-ray:

Please consider:
1. The ROA formula can be a simple, sophisticated, and rapid x-ray evaluation of behavior: what one is or is not doing.
2. Metabolic energy that is confined to two areas can be problematic.
3. Each one of us is a tree in the forest of mankind. To be able to smell the roses might oblige us to use a formula such as the ROA to examine and heal problematic behavior of ourselves and our forest.
4. The integration of psychiatry and medicine has great potential to maneuver metabolic energy. It led to removal of a patient’s delusion that she was pregnant.
(1) Paltrow KG, Brophy JJ. Review of areas: A Key to diagnosis. McGraw-Hill, Inc. Postgraduate Medicine 42: A 137-A 141, December 1967©
(2) Paltrow KG. Review of areas: Updated method of patient evaluation. McGraw-Hill, Inc. Postgraduate Medicine Vol 67/NO 1: 211-215 Jan 1980©.